Key Takeaways
- 迅速な高感度トロポニンT(hs-TnT)の0h/1hアルゴリズムは、急性心筋梗塞(AMI)を速やかにルールアウトする上で役立ちます。
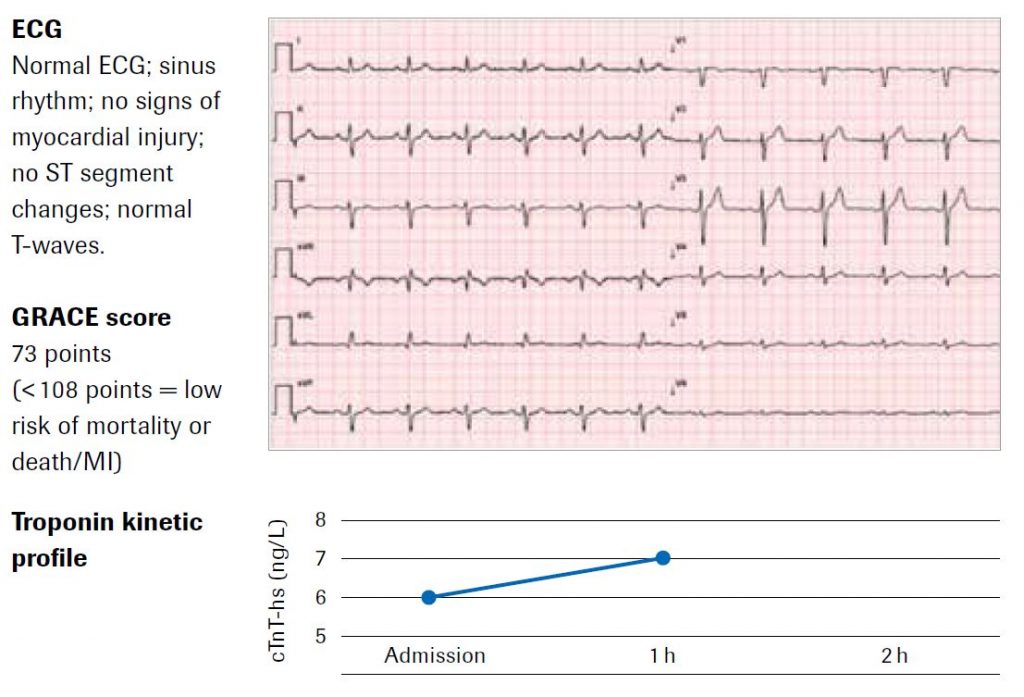
- hs-TnT値をGRACEスコアおよび心電図(ECG)と組み合わせると、その後の死亡リスクが低いかどうかを予測する上で役立ちます。
- hs-TnTの0h/1hアルゴリズムを用いたAMIの早期ルールアウトは、侵襲的な血管造影の使用を減らし、費用や医療資源の利用を減らす上で役立ちます。


.hidecontent { display:none; }
setTimeout(function(){
$(document).ready(function() {
$(“.readmorebtn”).find(‘a’).click(function() {
$(“.hidecontent”).show();
$(“.readmorebtn”).hide();
});
});
}, 3000);
推奨される手順
確立されたリスクスコア(例:GRACE 2.0スコア)のいずれかに基づいてリスクを層別化します(エビデンスレベル IB)。
心エコー検査(エビデンスレベル IC)およびマルチスライスCT検査(エビデンスレベル IIaA)により鑑別診断評価をします:「筋骨格系由来または不安定狭心症など」
症状の訴えのない患者では、攣縮性狭心症などの特別な状況を除き、モニタリングは不要です(エビデンスレベル IIbC)。
患者に症状がなく、リスクパラメータを1つも示さない限り、ルーチンの侵襲的冠動脈造影の適応とはなりません。
退院が可能で、外来時にストレス試験(エビデンスレベル IA)および冠動脈CT検査を含む精密検査を行います。
結論
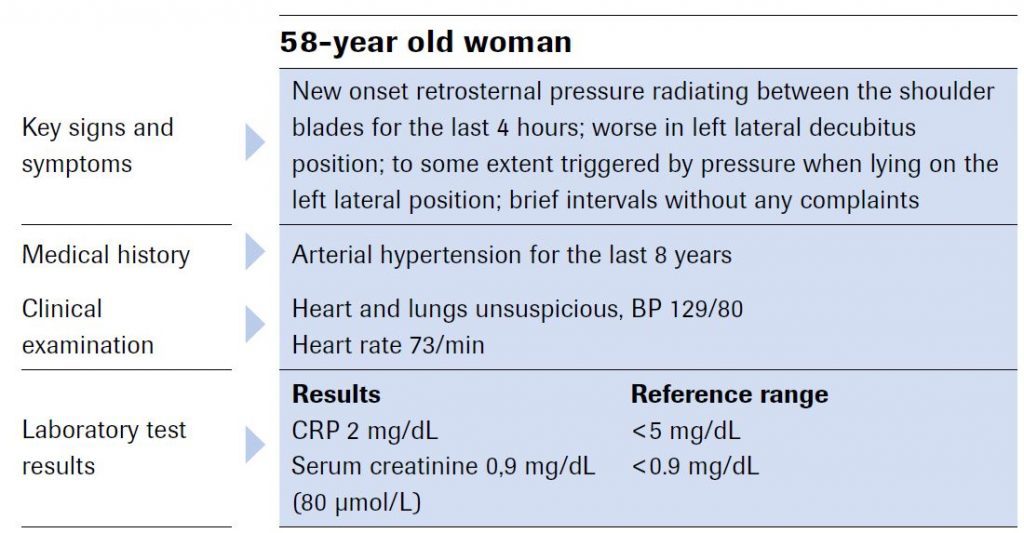
欧州心臓病学会(ESC)の2015年版ガイドラインの基準によると、0h/1hアルゴリズムを用いることで、非ST上昇型心筋梗塞(NSTEMI)をルールアウトできます(初期トロポニン値が12 ng/L未満で、1時間以内に上昇が
著者の見解
迅速な意思決定のために早期診断が必要な場合、cTnT-hsを用いた0h/1hアルゴリズムの方が、標準的な0h/3hまたは0h/6hアルゴリズムよりも推奨されます。